Latest Drugwonks' Blog
Mom, Apple Pie, and NIH Funding
Is NIH funding really the be-all/end-all of healthcare innovation?
Mari Serebrov, Washington Editor of BioWorld writes, “With the sequestration blade set to indiscriminately shave federal programs again in January, a bipartisan group of senators is urging congressional budget negotiators to spare research dollars at the National Institutes of Health (NIH).”
But is NIH really the only game in town.
Such a singular focus on the basic research funded by NIH ignores the fact that other government agencies are doing important health care research, Peter Pitts, president of the Center for Medicine in the Public Interest, told BioWorld Today. That research also is getting nicked by the sequester razor.”
For instance, the FDA funds research into regulatory science and personalized medicine, despite a “very limited budget,” Pitts said. While regulatory science research may not seem as sexy as basic research into cancer cures, it’s necessary research, he added.
“Basic research is important,” Pitts said, “but it’s not the beginning, middle and end” of all health care research.
The concerns also ignore new government funding for other types of research. Pitts described the current U.S. funding of public health-related research as “a bigger pie with more people with knives and forks.” More research is taking place, but the NIH slice of the pie isn’t getting any larger.
A prime example of that growth was the creation of the Patient-Centered Outcomes Research Institute (PCORI) in 2010. Set up as a nonprofit under the Affordable Care Act, PCORI was charged with funding comparative-effectiveness research. While Congress began shaving NIH funding close to the jaw line, it mandated that $10 million be set aside in fiscal 2010 to fund PCORI’s activities, $50 million in fiscal 2011 and $150 million in fiscal 2012.
To date, PCORI, which is funded through transfers from two Medicare trust funds rather than general tax dollars like the NIH, has approved 197 research awards totaling more than $273.5 million. It also is committing more than $1 billion to research funding over the next two fiscal years. But that money will be used to “study other people’s research, rather than the basic research NIH promotes,” Pitts said.
Noting that all research is subjective, Pitts said it isn’t Congress’ job to approve individual research projects, but Congress makes the choices of how federal research dollars are spent in general.
The complete BioWorld article can be found here.
According to Peggy Hamburg ...
The difference between science and science fiction is a line that seems ever harder to distinguish, thanks in part to a host of astonishing advances in medical science that are helping to create a new age of promise and possibility for patients.
Today cancer drugs are increasingly twinned with a diagnostic device that can determine whether a patient will respond to the drug based on their tumor’s genetic characteristics; medical imaging can be used to identify the best implantable device to treat a specific patient with clogged coronary arteries; and progress in regenerative medicine and stem cell therapy using a patient’s own cells could lead to the replacement or regeneration of their missing or damaged tissues. Given these trends, the future of medicine is rapidly approaching the promising level of care and cure once imagined by Hollywood in futuristic dramas like Star Trek.
But these examples are not science fiction. They are very real achievements that demonstrate the era of “personalized medicine” where advances in the science of drug development, the study of genes and their functions, the availability of increasingly powerful computers and other technologies, combined with our greater understanding of the complexity of disease, makes it possible to tailor treatments to the needs of an individual patient. We now know that patients with similar symptoms may have different diseases with different causes. Individual patients who may appear to have the same disease may respond differently (or not at all) to treatments of that disease.
FDA has been playing a critical role in the growth of this new era for a number of years. Even before I became FDA Commissioner the agency was creating the organizational infrastructure and putting in place the regulatory processes and policies needed to meet the challenges of regulating these complex products and coordinating their review and oversight. It has been my pleasure to serve at FDA during this next exciting period and to help ensure that the agency continues to prioritize this evolution by anticipating, responding to, and encouraging scientific advancements.
I am very pleased to be able to present a new report by FDA as part of our ongoing efforts in this field. Paving the Way for Personalized Medicine: FDA’s Role in a New Era of Medical Product Development describes many of the exciting developments and looming advances in personalized medicine, lays out the historical progress in this field, and examines FDA’s regulatory role: from ensuring the availability of safe and effective diagnostic devices, to addressing the challenges of aligning a drug with a diagnostic device, to post-market surveillance.
Outside collaboration and information sharing is essential for this field to flourish. On Tuesday, the American Association for Cancer Research and AdvaMedDX held a fruitful daylong conversation on personalized medicine to treat cancer. I was one of the speakers, participating in a conversation with Dr. Francis Collins, the head of the National Institutes of Health. Our discussion focused in part on current status of drug and diagnostic co-development and the challenges and potential of whole genome sequencing, where data can be collected on a patient’s entire genetic makeup at a reasonable cost in a reasonable amount of time.
FDA is committed to fostering these cooperative efforts, as it will require the full force of government, private industry, academia and other concerned stakeholders to maximize our efforts and fully realize the promise of personalized medicine. Our new report outlines that commitment, and helps chart the way forward so that more people can live long and prosper.
Via the New Republic:
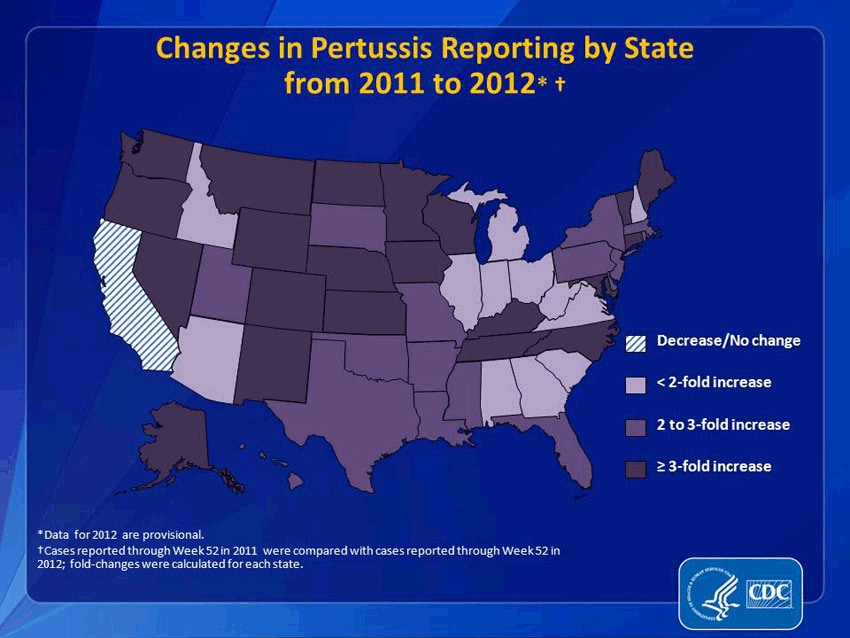
It would be an understatement to say that pertussis and other formerly conquered childhood diseases like measles and mumps are making a resurgence. Pertussis, specifically, has come roaring back. From 2011 to 2012, reported pertussis incidences rose more than threefold in 21 states. (And that’s just reported cases. Since we’re not primed to be on the look-out for it, many people may simply not realize they have it.) In 2012, the CDC said that the number of pertussis cases was higher than at any point in 50 years. That year, Washington state declared an epidemic; this year, Texas did, too. Washington, D.C. has also seen a dramatic increase. This fall, Cincinnati reported a 283 percent increase in pertussis. It’s even gotten to the point that pertussis has become a minor celebrity cause: NASCAR hero Jeff Gordon and Sarah Michelle Gellar are now encouraging people to get vaccinated.
How responsible are these non-vaccinating parents for my pertussis? Very. A study recently published in the journal Pediatrics indicated that outbreaks of these antediluvian diseases clustered where parents filed non-medical exemptions—that is, where parents decided not to vaccinate their kids because of their personal beliefs. The study found that areas with high concentrations of conscientious objectors were 2.5 times more likely to have an outbreak of pertussis. (To clarify: I was vaccinated against pertussis as a child, but the vaccine wears off by adulthood, which, until recently, was rarely a problem because the disease wasn't running rampant because of people not vaccinating their kids.)
So thanks a lot, anti-vaccine parents. You took an ethical stand against big pharma and the autism your baby was not going to get anyway, and, by doing so, killed some babies and gave me, an otherwise healthy 31-year-old woman, the whooping cough in the year 2013. I understand your wanting to raise your own children as you see fit, science be damned, but you're selfishly jeopardizing more than your own children. Carry your baby around in a sling, feed her organic banana mash while you drink your ethical coffee, fine, but what gives you denialists the right to put my health at risk—to cause me to catch a debilitating, humiliating, and frightening cough that, two months after I finished my last course of antibiotics (how’s that for supporting big pharma?), still makes me convulse several times a day like some kind of tragic nineteenth-century heroine?
If you have an answer, I’ll be here, whooping, while I wait.
Read the full article here.
According to a new letter to the British Medical Journal, “Doctors may not report adverse events or speak up when they witness poor care because of fear of punitive action or lack of confidence that reporting will change anything.”
Whose responsibility is it to build confidence in both the pharmacovigilance process as well as the urgent importance of the proposition? I believe it’s the job of the regulatory body that oversees the both the procedures and the actions that derive from post-marketing reports. That means (in the US), the FDA.
Would it be nice if the FDA could get additional dollars to ramp up pharmacovigilance beyond MedWatch and Sentinel? Sure, but let’s get real – that ain’t gonna happen. What the FDA does have at its disposal is the bully pulpit. It’s time for Janet, Peggy, and Gerald to get up on their soapboxes and start preaching the urgency and importance of pharmacovigilance.
Such renewed efforts are called for since the focus is now increasingly on patient outcomes. If we can’t measure it, it doesn’t count – or counts for less. Perhaps it’s time for the FDA to create an advisory committee of pharmacovigilance issues – and hold meetings to focus on process improvement, greater stakeholder involvement (not just with physicians, but with pharmacists, hospitals and patients), and better ways to share post-marketing data in a transparent and timely fashion – and not just adverse events and label updates but also Substandard Pharmaceutical Events (SPEs), when patient’s don’t respond as they should when their therapy has been impacted by therapeutic switching or interchangeability/bioequivalence issues.
Can you say, “biosimilars?” It's an adverse event horizon.
Sebelius & Co. have released enrollment numbers. Some key findings:
* 106,185 people have selected an Exchange plan (although not all have paid the premium). This includes 26,794 people in the federal exchange states.
* 396,261 people whose applications were processed by the Exchanges have been deemed eligible for Medicaid. A little more than half of those people live in states with state-based exchanges.
* Surprisingly, of those deemed eligible for Marketplace plan enrollment, only 30% qualified for a premium tax credit. CBO had expected about 80% of Exchange enrollees would qualify for a premium tax credit.
* About a million people have been deemed eligible for Exchange coverage but have not yet picked a plan. It’s not clear if these people will pick a plan later on or decided not to enroll – especially if their “cancelled” plans are reinstated.
* The HHS release includes a long appendix comparing Exchange enrollment to Part D, Massachusetts Commonwealth Care, CHIP and FEHBP. While Part D had about 10% enrollment in the first month, Massachusetts had just 3% enrollment in the first month (and the Bay State kept enrollment open for the entire first year so there was less pressure to enroll early).
* If exchange enrollment mirrors the same enrollment pattern as Part D, about 700,000 people would have to enroll by the end of November in order to meet the target of 7,000,000 people enrolled in Exchanges in 2014.
And speaking of exchanges, Gallup has found that just 18% of uninsured adults had attempted to visit an Exchange website.
Technical notes:
* This report only captures enrollment through Nov 2.
* Data includes applications submitted through methods other than the website (i.e. paper applications).
* There are state-by-state tables included in the release (see page 9).
The complete HHS release can be found here.
The term “context of use” refers to a comprehensive description that fully and clearly delineates the limits of FDA’s qualification decision in terms of the manner and purpose of use for the DDT(s). The context of use statement should describe all criteria under which the DDT is qualified for use. The qualified context of use defines the boundaries within which the available data adequately justify use of the DDT(s). As data from additional studies are obtained over time, submitters of DDTs may continue working within the DDT Qualification Programs to submit additional data and expand the qualified context of use.
http://www.fda.gov/Drugs/DevelopmentApprovalProcess/DrugDevelopmentToolsQualificationProgram/
What is Qualification?
Qualification is a conclusion that within the stated context of use, the DDT can be relied upon to have a specific interpretation and application in drug development and regulatory review. Once qualified, DDTs will be publicly available to be used in any drug development program for the qualified context of use. The qualified DDT can be included in IND or NDA/BLA submissions without the need for CDER to reconsider and reconfirm the suitability of the DDT as long as:
* There are no serious study flaws
* There are no attempts to apply the DDT outside the qualified context of use
* There are no new and conflicting scientific facts not known at the time the qualification was determined
Qualification may contribute to acceptance and application of DDTs across multiple drug development programs. Having qualified DDTs that can be utilized by many sponsors will aid in optimizing drug development and evaluation.
These Qualification Programs promote a collaborative setting in which there are advantages for multiple interested parties to work together in a consortium to develop DDTs for qualification. Resources and knowledge-sharing outside a specific drug development program can accelerate DDT development and facilitate availability of DDTs at critical milestones for future drug development programs. Early and continued interactions with FDA during the DDT development process are critical to the success of these programs.
Regulators love ambiguity because it gives them power. But flexibility is important. All this to say, it’s a tough balance.
And, once again, context matters.
From the pages of The Washington Examiner ...
Here comes the next big healthcare disaster, courtesy of HHS
And you thought the rollout of Obamacare was a catastrophe?
Here’s an immediate and critical pending national healthcare disaster — a new flu pandemic with nobody home at the Department of Health and Human Services.
This past April, a new strain of H7N9 avian influenza emerged in China and quickly spread throughout the region.
Though the H7N9 virus was only known to transfer directly from an avian source, numerous people were exposed to the disease’s devastating illnesses.
By the time the virus had momentarily vanished in August, a staggering 44 of the 134 infected had died, a 33 percent mortality rate.
At first, HHS took the necessary steps to address the new pandemic and prepare for the worst. Health and Human Services Secretary Kathleen Sebelius determined that the virus was a threat to U.S. national security and to Americans living abroad.
Subsidiary offices of HHS, the Biomedical Advanced Research and Development Authority and the Centers for Disease and Control, recommended producing a seed vaccine, conducting clinical trials and, if the threat of pandemic remained, contracting manufactures to produce vaccine stockpiles.
Once the virus was identified as a legitimate threat, HHS moved quickly to contract with vaccine manufacturers to produce a vaccine and prepare for mass production if the virus was to resurface, as influenza viruses typically do.
It seemed as though the government was taking on this threat appropriately — until Sebelius’ slogging bureaucracy, those wonderful people who brought you Obamacare, took over.
In September, BARDA contracted three vaccine manufacturers for $110 million to put in order a vaccine and prepare mass vaccine stockpiles once HHS gave them the go-ahead.
Reportedly, HHS was supposed to provide the manufacturers with further instructions by mid-October.
Yet today, HHS still sits on the very production orders that are necessary to stockpile the H7N9 vaccine to protect against a pandemic.
HHS’s timing could not be worse, with flu season already upon us. As of this week, there have been four newly reported cases of the H7N9 virus in China, leading a spokesman for the World Health Organization to conclude succinctly: "Winter is starting."
While experts have stopped short of guaranteeing a spike in H7N9 cases, the threat of a pandemic is anything but far-fetched.
If the second phase of this virus evolves from an avian-transferred virus to a human-to-human transfer, we will see devastating results.
Perhaps staff at HHS should heed the words of their colleague, Dr. Tom Frieden, director of the CDC.
In September, Frieden warned that “nothing has the potential to kill more people than influenza. A strain such as H7N9 could create a pandemic. When something with that much potential to cause widespread harm emerges, we must identify it in hours or days, not weeks or months.”
It will take, at minimum, 60 days to produce the first wave of vaccine stockpiles once an order is given to vaccine manufacturers.
And that is just the first wave, a quantity that would be wholly insufficient for the American public at large. Protecting the entire U.S. population would take many months, time that, frankly, we may not have.
Unfortunately, now HHS has again demonstrated gross incompetence in its obligation to best promote the public health. Its eye is not on the prize of pandemic preparedness.
If the federal bureaucracy continues to stall on producing the H7N9 vaccine, HHS could face a catastrophe that would make the healthcare.gov storm seem like a light spring shower.
Peter Pitts, a former FDA associate commissioner, is president of the Center for Medicine in the Public Interest.
From the pages of Law360.com …
Iclusig Deaths Won't Stall FDA's Speedier Drug Approvals
By Jeff Overley
The jarring death toll linked to leukemia drug Iclusig will force the U.S. Food and Drug Administration to revisit the science that won the product accelerated approval, but a growing willingness of seriously ill patients to accept risk means the tragic episode is unlikely to delay other fast-tracked medicines, experts say.
Sales of the chemotherapy drug, which earned FDA clearance in December, were halted last week after manufacturer Ariad Pharmaceuticals Inc. reported that at least 14 fatalities had occurred among 530 patients in two clinical trials. In addition, scores of other people suffered major side effects resulting from blood clots, including tissue death that led to amputations.
The dramatic circumstances add an important chapter to a long-running debate about FDA’s various “priority review” programs, which involve quicker analysis by regulators and may apply a relaxed safety standard.
While FDA is wary of risky medications, it’s increasingly under pressure from patients who say potentially dangerous treatments for deadly diseases are better than no treatments at all. That’s a trend with roots in the darkest days of the HIV/AIDS crisis, and it has only picked up steam in recent years.
“If someone has no options, it makes sense to try anything,” said Areta L. Kupchyk, a partner at Nixon Peabody LLP and former associate chief counsel for drugs and biologics at FDA.
Many drugs, even those approved on traditional pathways, are found to have more serious risks post-approval, but the Iclusig saga is particularly notable, as FDA rarely urges manufacturers to pull products from the market.
The development also comes at a time of rising scrutiny of whether the FDA has found the sweet spot in addressing unmet medical needs while continuing to protect patients from toxic medicines.
“It’s a very precarious balance,” said Peter J. Pitts, president and co-founder of the nonprofit Center for Medicine in the Public Interest.
For example, scholarly papers have explored whether standards are too loose. One article, published last year in the Journal of the American Medical Association, called particular attention to three products — AstraZeneca PLC’s cancer drug Caprelsa, Novartis AG’smultiple sclerosis medicine Gilenya, and Boehringer Ingelheim GmbH’s blood thinner Pradaxa — and asked whether their risk-benefit profiles made priority review inappropriate.
The safety record of the drugs raises the question “of whether it was good policy to approve three innovative new drugs with significant safety questions unanswered and with optimal doses not determined," according to the researchers Thomas Moore of the Institute for Safe Medication Practices and Dr. Curt Furberg, then of the Wake Forest University School of Medicine.
In a second article published just days before the freeze on Iclusig sales, the same authors found that drugs receiving expedited approval in 2008 typically used data from trials with less than one-fifth the usual number of patients and that progress was slow on completing mandatory post-approval studies.
In some recent years, nearly half the new drugs cleared by the FDA have used expedited pathways, raising the stakes should those routes be called into question by a review of Iculsig's approval.
“The question one has to ask is: Were there ... safety signals before this?” Kupchyk said. “That might be something that FDA and others wants to look at more closely.”
But while the events surrounding Iclusig are serious, experts say they don’t necessarily reflect poorly on priority review. FDA knew that blood clots were a risk at the time of approval and required a black box warning to that effect. It also ordered post-approval analysis that discovered greater-than-expected dangers less than one year after clearance, suggesting things worked largely as designed.
“What happened here seems to be consistent with the program, and I don’t see that FDA is going to pull back necessarily unless there is some evidence that they missed,” Kupchyk said.
FDA’s reaction with respect to its overall approach to expedited approvals is hard to predict because the amount of acceptable risk can vary greatly depending on which condition is being treated and whether there are any other effective drugs available.
“Safe is a relative concept. You wouldn’t approve a drug for allergies that is fatal for 30 percent of patients,” Pitts said.
Also, the prerogatives of distinct patient communities are influencing FDA more and more. Last year’s user-fee law directed the agency to refine its risk-benefit assessments, and a big part of that is so-called patient-focused drug development, which entails staging public meetings to gauge willingness to gamble on unproven drugs. Gatherings so far have covered chronic fatigue syndrome, HIV, lung cancer and narcolepsy, and more will take place involving fibromyalgia, sickle cell anemia and more than a dozen other conditions.
On Wednesday, an FDA spokeswoman defended the current system and did not directly answer a question about how the agency would decide whether any mistakes were made in approving Iclusig, which remains available in extremely narrow circumstances.
“We have a robust program for post-marketing surveillance and ensuring the benefits of a marketed drug outweigh its risks," FDA spokeswoman Stephanie Yao said. "If that profile changes in any way, we review and take appropriate action."
Regardless of whether anything should have been done differently with Iclusig, when dealing with the deadliest diseases and strong lobbying from people affected by them, experts say it may be inevitable that things occasionally go awry.
“When it comes to accelerated approval, it’s a high-risk, high-reward situation,” Pitts said. “The FDA’s not going to get it right all the time.”
From the pages of the New York Times …
Label Updates May Be Allowed for Generics
By KATIE THOMAS
The Food and Drug Administration proposed a rule on Friday that would permit generic drug makers to update their labels if they received information about potential safety problems. The move puts the companies on equal footing with brand-name manufacturers, but it also opens the door to lawsuits against them for the first time since the Supreme Court barred such cases two years ago.
Until now, only brand-name drug makers had the ability to independently update their labels if important new information surfaced about one of their drugs. If the F.D.A. agreed that the new information warranted a change in the label, then generic companies were required to update their product information so that it would be identical to the branded drug’s labeling.
Dr. Janet Woodcock, the F.D.A.’s head of drug evaluation and research, said the proposed change would create better parity between brand-name drug manufacturers and generic companies, which is especially important given that more than 80 percent of prescriptions in the United States are currently dispensed as generic drugs. “Now, with the generic industry having grown up, most people are taking generic drugs,” she said in a telephone interview. “It’s really time to level the playing field.”
The rule would also pave the way for lawsuits from patients who could now claim that generic companies did not sufficiently warn them of a drug’s dangers. In 2011, the Supreme Court ruled that such lawsuits were not valid because generic companies were required to use the same label warnings as brand-name manufacturers and thus could not be blamed for failing to warn patients about the risks of taking their drugs.
Consumer advocates, who have long called on the agency to make such a change, praised the decision because they said the current situation was unfair to patients harmed by generic drugs.
“This is an important consumer protection provision,” said Representative Chris Van Hollen, Democrat of Maryland, who had supported such a change. “It’s a long time in coming.”
The Generic Pharmaceutical Association, the industry trade group, said it was still reviewing the regulation but was concerned that the change could create confusion. In a statement, Ralph G. Neas, the association’s president, said the group was “very concerned that multiple versions of critical safety information would lead to unnecessary confusion and uncertainty for prescribers and other health care professionals, with harmful consequences for patients.”
Mr. Neas also raised the question of whether the rule was legal. “The Supreme Court has repeatedly held that generic pharmaceutical manufacturers must duplicate the language on the brand pharmaceutical manufacturer’s labels and cannot make changes to a label without F.D.A. approval,” he said in the statement. “Therefore, the agency’s authority to enact a rule that differs from the federal law is unclear.”
The proposed rule, which is open to public comment for 60 days, would set up a website that would place all updates for a given drug in one place, minimizing such confusion, Dr. Woodcock said.
The agency said the Supreme Court decision, Pliva v. Mensing, altered the incentives for generic drug companies to conduct adequate monitoring of their drugs because it eliminated the threat of lawsuits from patients who were harmed by those products. In proposing the rule, the agency said it “intended to ensure that generic drug companies actively participate with F.D.A. in ensuring the timeliness, accuracy and completeness of drug safety labeling.”
Dr. Woodcock said she did not expect that generic companies would update their labels frequently, because by the time drugs become available as generics, they have been on the market for years. “It’s not to say that we won’t learn new things, but it becomes less likely to come across new serious adverse events,” she said.To address (one hesitates to say “celebrate”) American Diabetes month, here is the latest addition to Pfizer’s Value of Medicines series -- The Value of Medicine for Type 2 Diabetes.
The development of medicines is complicated -- explaining their value should not be. Pfizer's straightforward efforts put the facts in perspective -- and in plain English. Their Value of Medicines series provides highly valuable tools for healthcare policy professionals, practitioners, and patients. Additional materials can be found here.
Knowledge is Power.
Center for Medicine in the Public Interest is a nonprofit, non-partisan organization promoting innovative solutions that advance medical progress, reduce health disparities, extend life and make health care more affordable, preventive and patient-centered. CMPI also provides the public, policymakers and the media a reliable source of independent scientific analysis on issues ranging from personalized medicine, food and drug safety, health care reform and comparative effectiveness.




{kind=link}